763
Views & Citations10
Likes & Shares
Aim: To
evaluate treatment patterns, cumulative survival and long-term effectiveness of
biologic disease-modifying anti-rheumatic drugs (bDMARD) in patients with
Psoriatic Arthritis (PsA).
Materials
and methods: Observational retrospective multicentre study. Patients
diagnosed with PsA treated with bDMARDs were included. Socio-demographic and
clinical data was collected. We gathered information on bDMARD start date,
concomitant treatment, suspension or change in treatment, and reasons for
discontinuation. Therapeutic response was defined according to MDA (Minimal
Disease Activity) at 6 and 12 months and then annually since the beginning of
bDMARD treatment.
Statistical
analysis: Student and Chi-square Test; Kaplan Meier and Log
Rank curves; Cox regression analysis.
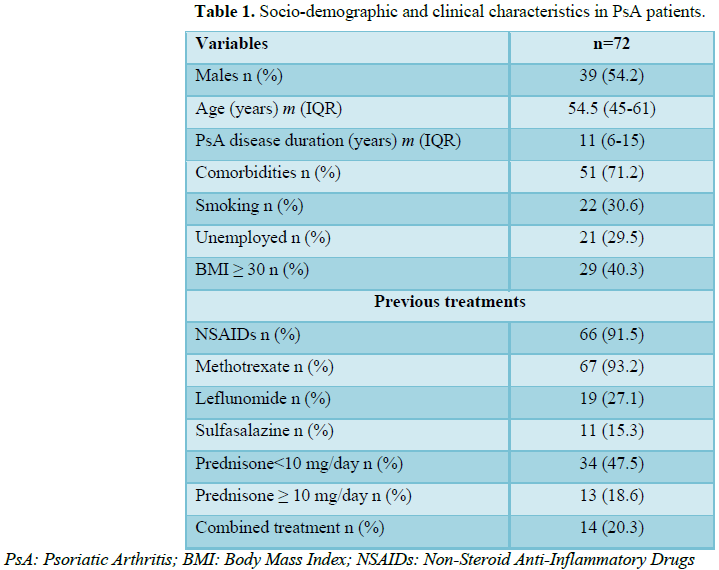
Results: 72 PsA
patients were included, 39 (54.2%) were male. Median age was 54.5 years (IQR
45-61) and median disease duration was 11 years (IQR 6-15). 71.2% of patients
presented comorbidities. bDMARs used in decreasing order of frequency were
Adalimumab (45.83%), Etanercept (36.1%), Certolizumab (5.6%), Infliximab
(4.2%), Ustekinumab (4.2%), Abatacept (2.7%) and Golimumab (1.4%). 15 patients
(25.4%) received bDMARD as monotherapy. Mean bDMARD survival was 82 months (SD
± 7.4), without significant differences between the different agents. Older
patients had a shorter drug survival (≥ 55 years: X ̅ 59.8 (SD ± 10.5) vs.
<55 years: X ̅ 101.2 (SD ± 9.7), p=0.006), which remained significant after
adjusting for different confounders in the Cox regression analysis [(HR=1.064
(IC=1.01-1.11) p=0.005)]. The LUNDEX of the first biologic agent was 24.7% at 6
months and 44.3% at 12 months. LUNDEX was lower in obese patients (16% vs. 66%
at 1 year, p=0.89; 10.5 vs. 74.9% at 2 years, p=0.011 and 5.9 vs. 81.8% at 3 years,
p=0.005).
Conclusion: The
average survival of the first bDMARD was 6.8 years. Older age was the only
variable associated to shorter survival.
Keywords:
Psoriatic arthritis, Treatment patterns, Cumulative survival, Anti-rheumatic
drugs
INTRODUCTION
To the best of our knowledge there are no
studies in our country estimating biologic survival rates in patients with PsA
and studies of this type in Latin America are very scarce. Therefore, the aim
of this study was to evaluate bDMARD treatment patterns in PsA patients, as
well as to determine the survival rate of the first bDMARD, causes for
discontinuation and the variables associated with their survival.
MATERIALS AND
METHODS
A retrospective multicentre study was carried
out (PATTERNS-PsA study). Patients ≥ 18 years old, diagnosed with PsA according
to CASPAR criteria [17], who received treatment with bDMARDs during the course
of their disease were included. Socio-demographic data (age, sex, marital
status, education, occupation, health coverage), disease duration, clinical PsA
type (olygoarticular, polyarticular or mixed) and associated comorbidities were
recorded. Data regarding previous treatments causes for discontinuation and
concomitant treatments with bDMARD were also documented. Additionally, baseline
data was collected at the moment prior to the start of the first bDMARD
treatment, at 6 months and then annually. Height (cm) and weight (kg) were
recorded and Body Mass Index (BMI) was calculated. Disease activity was
measured by 66/68 swollen and painful joints [18], physician and patient
assessments of pain and disease activity by means of a Visual Numeric Scale
(VNS) [19]. Acute phase reactants were registered (ESR -mm/h- and CRP -mg/dl-).
Minimal Disease Activity (MDA) [20] was considered as a criteriaas a criterion
of treatment response. The LUNDEX index was used in order to evaluate drug
survival and effectiveness simultaneously [21]. This index results from the
product of the proportion of patients which continued a given bDMARD and the
proportion of patients fulfilling MDA criteria at the same time.
STATISTICAL ANALYSIS
Categorical variables were expressed as
frequencies and percentages, while continuous variables as mean and median with
their corresponding standard deviation (SD) or interquartile range (IQR).
Categorical variables were compared using the Chi Square test and continuous
variables by Student T test or Mann Whitney test according to their
distribution. Cumulative drug survival was analyzed using Kaplan Meier curves
and comparisons using Log Rank test. Variables associated to bDMARD survival
were analyzed using Cox regression analysis using survival as a time variable,
drug permanence as a dependent variable and various demographic, clinical and
therapeutic factors as independent variables. Up to 15% of missing data was
solved through data imputation by means of linear interpolation. A p value
<0.05 was considered significant.
RESULTS
DISCUSSION
Our results show an average survival of
biologic therapy of approximately 7 years in patients with PsA, with greater
survival for Adalimumab, but without significant differences. The only variable
associated to less survival was patient age ≥ 55. There was a trend to lower
survival in obese patients; nevertheless the LUNDEX was significantly lower in
those patients. In our study, Adalimumab was the first bDMARD most frequently
used, data which coincides with the DANBIO and ROB-FIN registers [5,9].
According to our results, Adalimumab presented a longer survival in comparison
to Etanercept, which differs from other studies that have shown that Etanercept
was the TNFi agent with the highest survival rate [14-16]. In the Finnish
register, Adalimumab survival was only superior to Infliximab, while it did not
differ to the survival of Etanercept or Golimumab [9]. Similar to the DANBIO
register, in our study the main cause for drug discontinuation was lack of
efficacy [5]. The second most frequent cause of discontinuation in our study
was the lack of provision, which is usually the result of irregularities by the
supplying institution of the medication, causing the stoppage of the treatment
beyond the patients’ will. A non-frequent variable in studies conducted in
developed countries.
Some studies have observed that concomitant
csDMARD use in patients treated with TNFi agents favored survival. The Danish
register proved that the lack of concomitant Methotrexate in patients treated
with bDMARD was associated to less drug survival [5]. Likewise, in the Swedish
register the same results were found, determining that concomitant use of
csDMARD paradoxically decreased the frequency of adverse events [6]. An Italian
study evaluating 8 year-long treatment with TNFi found that concomitant use of
Methotrexate was associated to a lower risk of bDMARD discontinuation [15]. In
our study, the use of csDMARD showed no influence on biologic survival. In
contrast to other studies, we found that patient’s ≥ 55 years old presented a
significantly lower survival to TNF inhibitors. In the DANBIO register, young
patients presented a better response to treatment, but not a greater survival
[5].⁵ According to the BIOBADASER register, which evaluated patients with
Spondyloarthritis including 570 patients with PsA, patients >60 years old
(HR=1.21), females, and those treated with Infliximab had a higher risk of
discontinuing bDMARD treatment [12]. Though the design of our study does not
allow us to know the causes leading to lower survival in these patients, one
could hypothesize that longer disease duration, higher number of comorbidities,
concomitant drugs, risks of infections and functional impairment or disability
may have some impact on drug survival.
Despite obese patients (BMI ≥ 30) had a
tendency towards lower bDMARD survival in univariate analysis, the LUNDEX was
significantly lower for obese patients after the second year of treatment.
These results are similar to those observed in CORRONA register, in which a
high BMI was found to be a significant predictor of a lower drug survival [22].
Our study has some limitations. First, the
number of patients included is relatively small, secondly, some biological
agents were administered to a low percentage of patients impeding their
separate analysis, and lastly, some data may be biased given that it is a
retrospective cohort.
MDA was used to estimate treatment response;
this differs to most studies which consider ACR response criteria. We decided
to use this outcome measure as it is a simple and accessible tool that takes
into consideration not only articular but extra-articular manifestations of this
disease.
One of the strengths of our study is that, to
the best of our knowledge, it is the first in our country to provide
information regarding biologic treatment survival in patients with PsA. Another
advantage is that it reflects a wide socioeconomic spectrum given that the data
corresponds to patients from diverse health centers, both public and private.
An additional advantage was the use of LUNDEX index to evaluate simultaneously
evaluates drug survival and effectiveness.
CONCLUSION
1. Chandran
V, Raychaudhuri SP (2010) Geoepidemiology and environmental factors of
psoriasis and psoriatic arthritis. J Autoimmun 34: 314-321.
2. Boehncke
WH, Menter A (2013) Burden of disease: Psoriasis and psoriatic arthritis. Am J
Clin Dermatol 14: 377-388.
3. Krueger
G, Koo J, Lebwohl M, Menter A, Stern RS, et al. (2001) The impact of psoriasis
on quality of life: Results of a 1998 national psoriasis foundation
patient-membership survey. Arch Dermatol 137: 280-284.
4. Ash
Z, Gaujoux-Viala C, Gossec L, Hensor EM, FitzGerald O, et al. (2012) A
systematic literature review of drug therapies for the treatment of psoriatic
arthritis: Current evidence and meta-analysis informing the EULAR
recommendations for the management of psoriatic arthritis. Ann Rheum Dis 71:
319-326.
5. Glintborg
B, Ostergaard M, Dreyer L, Krogh NS, Tarp U, et al. (2011) Treatment response,
drug survival and predictors thereof in 764 patients with psoriatic arthritis
treated with anti-tumor necrosis factor alfa therapy: Results from the
nationwide Danish DANBIO registry. Arthritis Rheum 63: 382-390.
6. Kristensen
LE, Gulfe A, Saxne T, Geborek P (2008) Efficacy and tolerability of anti-tumor
necrosis factor therapy in psoriatic arthritis patients: results from the South
Swedish Arthritis Treatment Group register. Ann Rheum Dis 67: 364-369.
7. Saad
AA, Ashcroft DM, Watson KD, Hyrich KL, Noyce PR, et al. (2009) Persistence with
anti-tumor necrosis factor therapies in patients with psoriatic arthritis:
Observational study from the British Society of Rheumatology Biologics
Register. Arthritis Res Ther 11: R52.
8. Virkki
LM, Sumathikutty BC, Aarnio M, Valleala H, Heikkila R, et al. (2010) Biological
therapy for psoriatic arthritis in clinical practice: Outcomes up to 2 years. J
Rheumatol 37: 2362-2368.
9. Aaltonen
K, Heinonen A, Joensuu J, Parmanne P, Karjalainen A, et al. (2017)
Effectiveness and drug survival of TNF-inhibitors in the treatment of psoriatic
arthritis: A prospective cohort study. Semin Arthritis Rheum 46: 732-739.
10. Heiberg
MS, Koldingsnes W, Mikkelsen K, Rodevand E, Kaufmann C, et al. (2008) The
comparative one-year performance of anti-tumor necrosis factor α drugs in
patients with rheumatoid arthritis, psoriatic arthritis and ankylosing
spondylitis: Results from a longitudinal, observational, multicenter study.
Arthritis Rheum 59: 234-240.
11. Saad
AA, Ashcroft DM, Watson KD, Symmons DP, Noyce PR, et al. (2010) Efficacy and
safety of anti-TNF therapies in psoriatic arthritis: An observational study
from the British Society for Rheumatology Biologics Register: Reply.
Rheumatology 49: 697-705.
12. Carmona
L, Gómez-Reino JJ (2006) Survival of TNF antagonists in spondylarthritis better
than in rheumatoid arthritis. Data from the Spanish registry BIOBADASER.
Arthritis Res Ther 8: R72.
13. Fagerli
KM, Lie E, van der Heijdee D, Heiberg MS, Kalstad S, et al. (2013) Switching
between TNF inhibitors in psoriatic arthritis: Data from the NOR-DMARD study.
Ann Rheum Dis 72: 1840-1844.
14. Saougou
I, Markatseli TE, Papagoras C, Voulgari PV, Alamanos Y, et al. (2011) Sustained
clinical response in psoriatic arthritis patients treated with anti-TNF agents:
A 5 year open-label observational cohort study. Semin Arthritis Rheum 40:
398-406.
15. Favalli
EJ, Selmi C, Becciolini A, Biggioggero M, Ariani A, et al. (2017) Eight year
retention rate of first-line tumor necrosis factor inhibitors in
spondyloarthritis: A multi-center retrospective analysis. Arthritis Care Res
69: 867-874.
16. Iannone
F, Lopriore S, Bucci R, Lopalco G, Chiala A, et al. (2016) Long-term clinical
outcomes in 420 patients with psoriatic arthritis taking anti-tumor necrosis
factor drugs in real-world settings. J Rheumatol 43: 911-917.
17. Taylor
W, Gladman D, Helliwell P, Marchesoni A, Mease P, et al. (2006) Classification
criteria for psoriatic arthritis: Development of new criteria from a large
international study. Arthritis Rheum 54: 2665-2673.
18. Gladman
DD, Helliwell P, Mease PJ, Nash P, Ritchlin C, et al. (2004) Assessment of
patients with psoriatic arthritis: A review of currently available measures.
Arthritis Rheum 50: 24-35.
19. Gladman
DD, Mease PJ, Strand V, Healy P, Helliwell PS, et al. (2007) Consensus on a
core set of domains for psoriatic arthritis. J Rheumatol 34: 1167-1170.
20. Coates
LC, Fransen J, Helliwell PS (2010) Defining minimal disease activity in
psoriatic arthritis: A proposed objective target for treatment. Ann Rheum Dis
69: 48-53.
21. Kristensen
LE, Saxne T, Geborek P (2006)The LUNDEX, a new index of drug efficacy in
clinical practice. Arthritis Rheum 54: 600-606.
22. Mease
PJ, Collier DH, Saunders KC, Li G, Kremer JM, et al. (2015) Comparative
effectiveness of biologic monotherapy versus combination therapy for patients
with psoriatic arthritis: Results from the Corrona registry. RMD Open 1:
e000181.
-
 Table 1
Table 1 -
Table 2




QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- BioMed Research Journal (ISSN:2578-8892)
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)
- Chemotherapy Research Journal (ISSN:2642-0236)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- Journal of Allergy Research (ISSN:2642-326X)


